Recognition of Complications After Pancreaticoduodenectomy for Cancer Determines Inpatient Mortality
DOI:
https://doi.org/10.6092/1590-8577/1883Keywords:
Intraoperative Complications, Morbidity, Mortality, PancreaticoduodenectomyAbstract
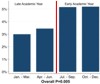
Context While perioperative mortality after pancreaticoduodenectomy is decreasing, key factors remain to be elucidated. Objective The purpose of this study was to investigate inpatient mortality after pancreaticoduodenectomy in the Nationwide Inpatient Sample (NIS), a representative inpatient database in the USA. Methods Patient discharge data (diagnostic and procedure codes) and hospital characteristics were investigated for years 2009 and 2010. The inclusion criteria were a procedure code for pancreaticoduodenectomy, elective procedure, and a pancreatic or peripancreatic cancer diagnosis. Chi-square test determined statistical significance. A logistic regression model for mortality was created from significant variables. Results Two-thousand and 958 patients were identified with an average age of 65±12 years; 53% were male. The mean length of stay was 15±12 days with a mortality of 4% and a complication rate of 57%. Eighty-six percent of pancreaticoduodenectomy occurred in teaching hospitals. Pancreaticoduodenectomy performed in teaching hospitals in the first half of the academic year were associated with higher mortality than in the latter half (5.5% vs. 3.4%, P=0.005). On logistic regression analysis, non-surgical complications are the largest predictor of death (P<0.001) while operations in the latter half of the academic year are associated with decreased mortality (P<0.01). Conclusions The timing of pancreaticoduodenectomy for cancer remained more predictive of mortality than age or length of stay; only complications were more predictive of death than time of year. This suggests that there remains a clinically and statistically significant learning curve for trainees in identifying complications; further study is needed to prove that identification of complications leads to a decrease in mortality rate by taking corrective actions.
Image: Inpatient mortality according to period of the academic year.
Downloads
References
Hoem, D. and A. Viste, Improving survival following surgery for pancreatic ductal adenocarcinoma--a ten-year experience. Eur J Surg Oncol, 2012. 38(3): p. 245-51.
Nitecki, S.S., et al., Long-term survival after resection for ductal adenocarcinoma of the pancreas. Is it really improving? Ann Surg, 1995. 221(1): p. 59-66.
Huguet, F., et al., Chemoradiotherapy in the management of locally advanced pancreatic carcinoma: a qualitative systematic review. J Clin Oncol, 2009. 27(13): p. 2269-77.
Squadroni, M. and N. Fazio, Chemotherapy in pancreatic adenocarcinoma. Eur Rev Med Pharmacol Sci, 2010. 14(4): p. 386-94.
Shrikhande, S.V., et al., Multimodality imaging of pancreatic ductal adenocarcinoma: a review of the literature. HPB (Oxford), 2012. 14(10): p. 658-68.
de Wilde, R.F., et al., Impact of nationwide centralization of pancreaticoduodenectomy on hospital mortality. Br J Surg, 2012. 99(3): p. 404-10.
Pecorelli, N., et al., Effect of surgeon volume on outcome following pancreaticoduodenectomy in a high-volume hospital. J Gastrointest Surg, 2012. 16(3): p. 518-23.
Schmidt, C.M., et al., Effect of hospital volume, surgeon experience, and surgeon volume on patient outcomes after pancreaticoduodenectomy: a single-institution experience. Arch Surg, 2010. 145(7): p. 634-40.
HCUP Nationwide Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). 2009-2010. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/nisoverview.jsp
Ahmad, S.A., et al., Factors influencing readmission after pancreaticoduodenectomy: a multi-institutional study of 1302 patients. Ann Surg, 2012. 256(3): p. 529-37.
Amini, A., et al., Effect of epidural analgesia on postoperative complications following pancreaticoduodenectomy. Am J Surg, 2012. 204(6): p. 1000-4; discussion 1004-6.
Clark, W., et al., Targeting early deaths following pancreaticoduodenectomy to improve survival. J Gastrointest Surg, 2012. 16(10): p. 1869-74.
Kim, S.Y., et al., Learning curve for a laparoscopic appendectomy by a surgical trainee. J Korean Soc Coloproctol, 2010. 26(5): p. 324-8.
Lekawa, M., et al., The laparoscopic learning curve. Surg Laparosc Endosc, 1995. 5(6): p. 455-8.
Maguire, T., et al., Analysis of the surgical learning curve using the cumulative sum (CUSUM) method. Neurourol Urodyn, 2013.